Your report has arrived — so what do the numbers actually mean? An omega-3 result is more readable than a standard blood panel once you know what each part is telling you. Here's a plain-English walkthrough of your Omega-3 Index, the reference ranges, the ratios on the fuller tests, and what to do depending on where you land.
Your Omega-3 Index: the headline number
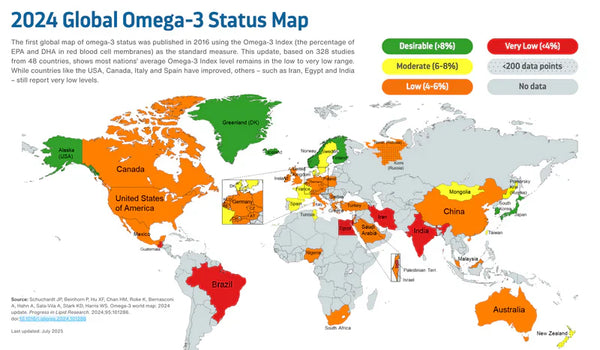
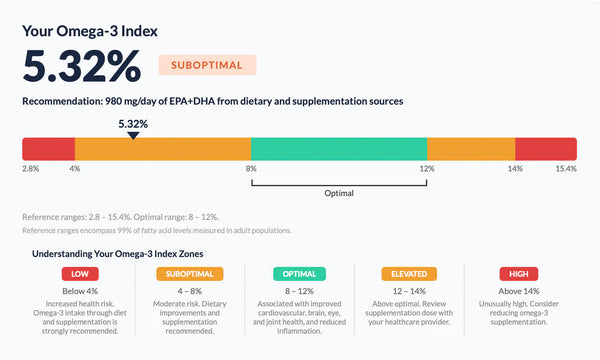
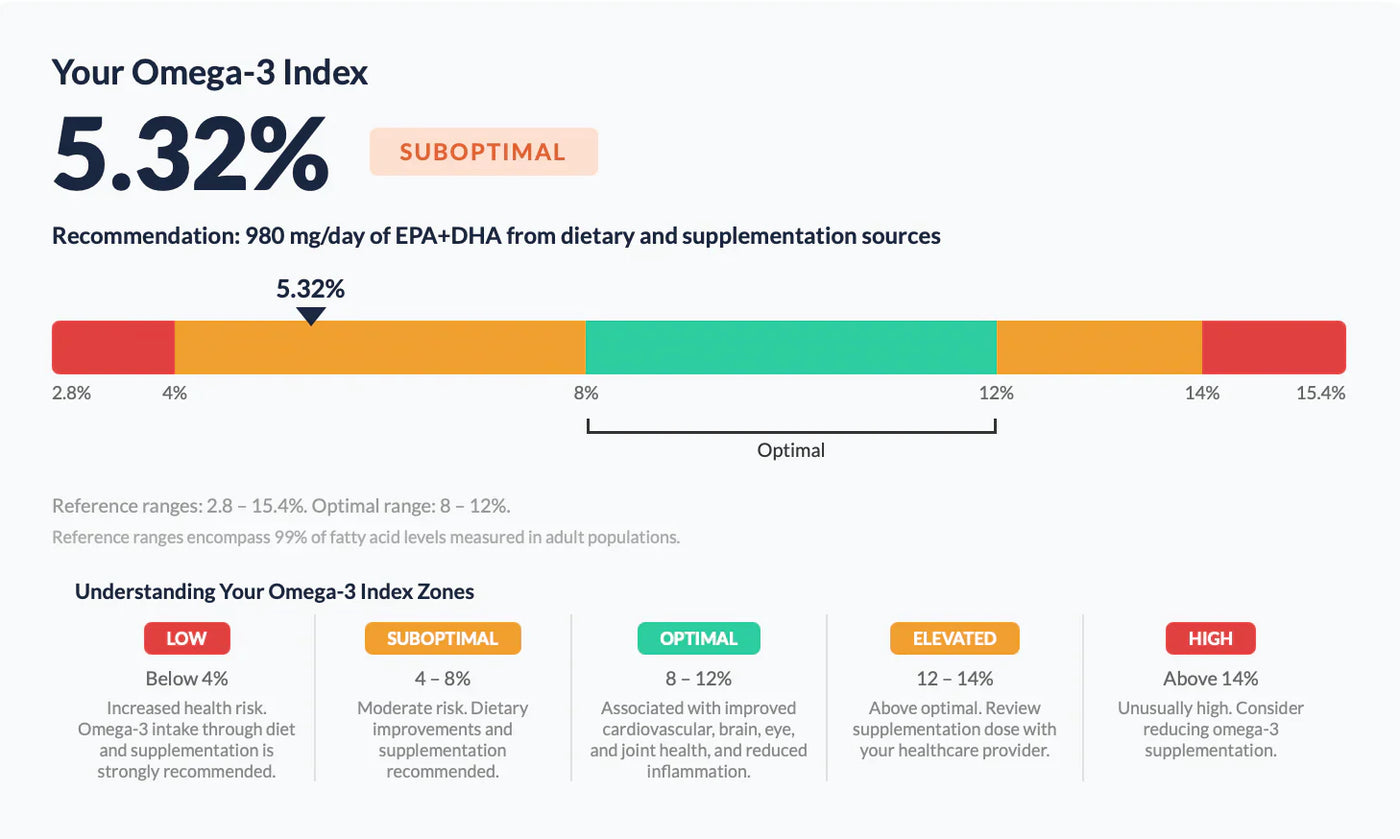
The figure most people look at first is the Omega-3 Index — your EPA plus DHA as a percentage of total red blood cell fatty acids. Because red blood cells turn over slowly, it reflects roughly the last three to four months, not a single meal. It's shown as a single percentage, usually plotted on a coloured scale.
Where you sit on the scale
- Below 4% — low: the band linked with the highest cardiovascular risk in observational studies.
- 4–8% — suboptimal: where most UK adults fall; there's room to improve.
- 8–12% — optimal: the target range proposed in the original research.
The aim is simply to move into, and stay in, the 8–12% band. If you're already there, the job becomes maintenance rather than catching up.
The ratios (on Plus Ratios and Complete)
If you took a test that includes ratios, you'll see two more numbers worth understanding:
Omega-6 : Omega-3 ratio
This compares how much omega-6 you carry relative to omega-3 — a marker of overall dietary fat balance. Modern Western diets tend to push this ratio high. The most effective way to improve it is usually to raise your omega-3 rather than fixate on cutting omega-6; our piece on the omega-6 to omega-3 ratio explains why.
AA : EPA ratio
This compares arachidonic acid (an omega-6) to EPA, and is often read as a more specific marker of inflammatory balance. As your EPA rises, this ratio typically narrows.
The EPA and DHA breakdown
Your report separates the two long-chain omega-3s. EPA and DHA do overlapping but distinct jobs — EPA features heavily in cardiovascular and inflammatory research, DHA is a structural fat concentrated in the brain and eyes. For most people the Index (the two combined) is the number that matters most; the split is useful context, especially if you're supplementing for a specific reason.
What to do if your result is low
A low or suboptimal result is common and very actionable. Broadly, raising your Index by one percentage point takes in the region of 370mg of EPA + DHA a day, sustained for several months (Walker et al., 2019) — so the further you are from target, the higher the daily amount. Our how much EPA and DHA guide turns that into a personalised figure, and the choosing a supplement guide covers form, dose and quality if you're not getting there from food alone.
What to do if your result is optimal
If you're in the 8–12% range, the goal is to hold it. That usually means continuing whatever got you there — regular oily fish or a steady supplement — and retesting periodically to confirm you've stayed put. There's no clear added benefit to pushing far above the optimal band.
When to retest
Because your red blood cells take three to four months to fully reflect a change, retesting sooner than that won't show the full effect. A practical rhythm is: baseline now, make your change, then retest at around three to four months to see whether it actually moved your number.
Frequently asked questions
What number am I aiming for?
An Omega-3 Index of 8–12%. Below that is suboptimal; there's no clear benefit to going far above it.
My Index is fine but my ratio looks high — which matters more?
The Omega-3 Index is the better-validated, more reproducible marker. Treat the ratio as useful context; raising your omega-3 generally improves both at once.
How soon will a change show up?
Allow three to four months. That's how long red blood cells take to reflect a new intake, so retesting earlier understates the effect.
Should I share my result with my GP?
Yes, if anything concerns you. The report is laid out like a pathology result so it's easy to discuss, though it provides information rather than a diagnosis.
Not tested yet? Get your baseline number first.
See our tests →References
- Harris WS, von Schacky C. The Omega-3 Index: a new risk factor for death from coronary heart disease? Preventive Medicine. 2004;39(1):212–220.
- Walker RE, Jackson KH, Tintle NL, et al. Predicting the effects of supplemental EPA and DHA on the omega-3 index. American Journal of Clinical Nutrition. 2019;110(4):1034–1040.
This article is general information, not medical advice, and the test is not a diagnostic test. Always discuss significant health decisions, or any changes to medication or supplements, with your GP.
Know your number.
A simple at-home finger-prick test, posted to your door. Find out where you actually stand on omega-3.
See our tests